Of all the factors that influence IQ and cognitive performance, nutrition is among the most consequential — and the most unevenly distributed around the world. The research on nutrition and intelligence covers a wide spectrum, from findings of extraordinary magnitude (iodine deficiency alone can reduce a child's IQ by 12–13 points on average, according to meta-analysis) to findings of modest effect (omega-3 supplementation in already well-nourished adults improves cognitive performance inconsistently and modestly).
The key distinction that makes this research tractable is the difference between deficiency correction and enhancement above adequacy. Correcting serious nutritional deficiencies during critical windows of brain development has some of the largest documented effects on IQ of any known intervention. Supplementing nutrients above adequate levels in already well-nourished individuals shows far weaker and less consistent effects. This distinction explains the apparent contradiction between dramatic population-level findings (iodine supplementation programs raising national IQ averages) and the disappointing results of "brain food" supplement trials.
This guide covers the full picture: the critical windows of brain development, the key nutrients with the strongest evidence, the magnitude of deficiency effects, and what the research actually supports for adults who want to protect and support their cognitive performance.
Why Timing Matters: Critical Windows of Brain Development
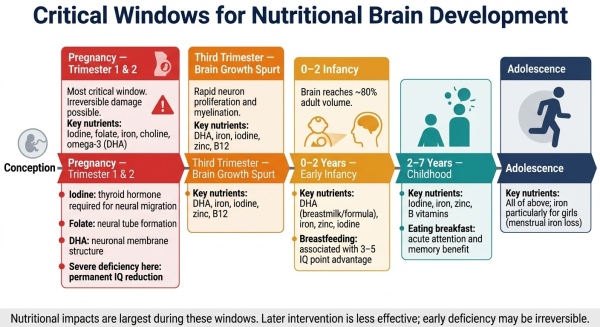
The brain is not equally sensitive to nutritional status throughout life. It passes through specific critical windows during which the cognitive impact of nutritional adequacy or deficiency is largest — and during which damage can be permanent. Understanding these windows is essential for interpreting the nutrition-IQ literature accurately.
The most critical window is pregnancy, particularly the first and second trimesters. During this period, the neural tube forms, neurons proliferate and migrate to their appropriate locations, and the fundamental architecture of the brain is established. Deficiencies in key nutrients during this window — iodine, folate, iron, omega-3 fatty acids (particularly DHA), zinc, and choline — can cause permanent structural and functional impairment that later supplementation cannot fully reverse.
The second critical window is the first two years of life, during which the brain reaches approximately 80% of its adult volume. Rapid myelination (the process by which nerve fibres gain the fatty sheaths that increase transmission speed), synaptic proliferation, and neurotransmitter system development all require adequate nutrition. Iron deficiency in this period is particularly well-documented as producing irreversible cognitive effects if severe or prolonged.
Early childhood through adolescence remains nutritionally important but less irreversibly critical: deficiencies during these periods impair cognitive performance and learning, but are more reversible with treatment than deficiencies during pregnancy and early infancy. For a framework on how cognitive ability measured later in life relates to these developmental foundations, see our guide on what IQ actually measures.
The Key Nutrients: Evidence Summary
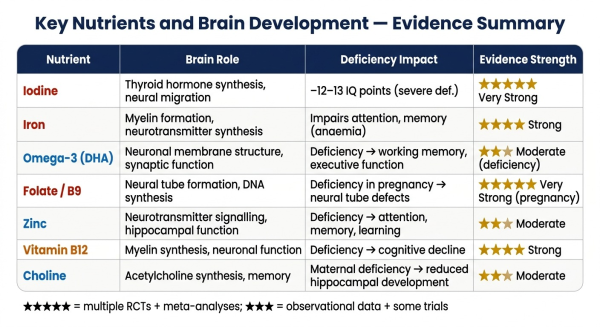
Iodine — The Strongest Single Nutritional Effect on IQ
Iodine deficiency is the leading preventable cause of cognitive impairment and brain damage worldwide, according to the World Health Organization. The evidence for its impact is among the most robust in all of nutritional neuroscience.
Iodine is required for the synthesis of thyroid hormones, which are essential regulators of brain development. Thyroid hormone directs neuronal migration, dendritic growth, myelination, and synaptogenesis. When a pregnant woman is iodine-deficient, her baby's brain development is compromised throughout the critical gestational window — and no amount of iodine supplementation after birth can fully reverse this.
The quantified evidence is striking. A meta-analysis by Bleichrodt and Born using studies from moderately to severely iodine-deficient areas estimated that iodine deficiency reduces IQ by an average of 13.5 points. A separate meta-analysis by Qian et al. (2005) on severely iodine-deficient populations in China found that children of iodine-deficient mothers scored approximately 12.3 IQ points lower than children of iodine-sufficient mothers. Salt iodisation programmes — cheap, population-scale, and well-studied — have reversed documented IQ deficits in multiple countries.
Even mild maternal iodine deficiency — with no obvious clinical symptoms — measurably reduces verbal IQ and reading performance in school-age children in several studies, though the evidence for mild deficiency is less consistent than for severe deficiency. For context on what a 13-point IQ difference means on the cognitive scale, see our guides on IQ 90 and IQ 105.
Iron — Essential for Myelin and Neurotransmitters
Iron plays critical roles in brain function: it is required for myelin synthesis (the fatty sheath around nerve fibres), for the production of key neurotransmitters (dopamine, serotonin, and norepinephrine), and for general oxidative metabolism in neurons. Iron deficiency anaemia — affecting a substantial proportion of children worldwide — is consistently associated with poorer performance on cognitive tests, particularly those measuring attention, working memory, and learning speed.
A meta-analysis by Falkingham et al. (2010) found that iron treatment improved IQ in children with iron deficiency anaemia — but iron supplementation did not improve IQ in non-anaemic children. This is a direct illustration of the deficiency-correction versus enhancement distinction: iron matters enormously when deficient, but supplementing above adequacy in non-deficient children produces no cognitive benefit.
If iron deficiency occurs in very early life (the first 1–2 years), the cognitive damage may be irreversible even with later iron treatment — a finding with significant implications for public health priorities.
Omega-3 Fatty Acids (DHA) — Important but Overstated in Well-Nourished Populations
Docosahexaenoic acid (DHA), the primary omega-3 fatty acid in the brain, is a major structural component of neuronal cell membranes and is essential for synaptic function. The brain is approximately 60% fat by dry weight, and DHA constitutes a substantial portion of cortical grey matter. This structural role makes it biologically plausible that DHA intake affects cognitive function.
The evidence is more nuanced than popular coverage suggests. Maternal DHA intake during pregnancy is associated with better neurodevelopmental outcomes in children — but a 2025 systematic review found that "the magnitude and consistency of these effects are modest and not uniform across all cognitive domains." Omega-3 supplementation studies in already well-nourished children and adults show inconsistent and generally small effects on IQ specifically. The benefit is clearest in populations with genuinely inadequate omega-3 intake.
Breastfeeding — which provides DHA in composition appropriate for brain development — is associated with a 3–5 IQ point advantage in multiple studies, though this association has been difficult to fully separate from the socioeconomic and care-quality confounds that also predict breastfeeding rates.
Folate / Vitamin B9 — Foundational for Neural Tube Formation
Folate is essential for DNA synthesis and neuronal proliferation in the developing embryo. Folate deficiency in early pregnancy is the best-documented cause of neural tube defects (anencephaly, spina bifida) — a finding that led to widespread folic acid fortification of staple foods and supplement recommendations for women planning pregnancy. The evidence for folate's role in cognitive outcomes beyond neural tube defects is more mixed, but adequate folate during pregnancy is clearly foundational for brain structural development.
Zinc, B12, Choline — Supporting Roles
Zinc is involved in neurotransmitter signalling, hippocampal function, and synaptic plasticity. Deficiency in children is associated with attention and learning difficulties. Vitamin B12 is essential for myelin synthesis and neuronal function; deficiency produces well-documented cognitive decline and neurological symptoms. Choline is the precursor for acetylcholine (the key memory neurotransmitter) and is essential for hippocampal development; maternal choline intake influences offspring hippocampal function in animal studies, with some human data supporting the association.
The Three Zones: Deficiency, Adequacy, and the Enhancement Illusion
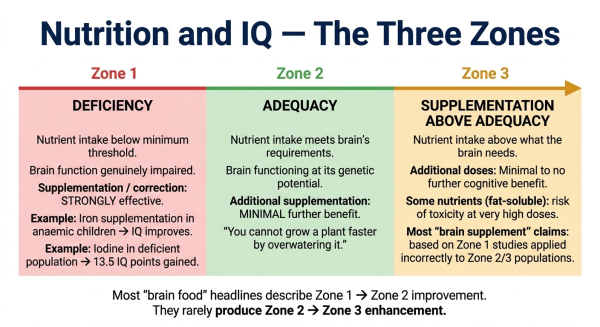
The most important conceptual framework for understanding the nutrition-IQ literature is the distinction between three nutritional zones:
Zone 1: Deficiency. Nutrient intake is below the minimum threshold for normal brain function. Correcting deficiency — through diet or supplementation — produces genuine and sometimes substantial cognitive improvements. The iodine and iron data reviewed above are the strongest examples: populations and individuals with genuine deficiency show real, measurable IQ and cognitive performance gains when the deficiency is corrected. This is where the dramatic headlines come from, and where the evidence is strongest.
Zone 2: Adequacy. Nutrient intake meets the brain's requirements. The brain is functioning at its nutritional baseline — at the level its genetic and environmental history allows. Additional supplementation above adequacy produces minimal or no further benefit on cognitive performance. You cannot grow a plant faster by overwatering it, and you cannot meaningfully enhance a brain that already has what it needs by adding more of the same nutrients.
Zone 3: Attempted enhancement above adequacy. Nutrient intake substantially above what the brain requires. For most water-soluble nutrients, excess is simply excreted. For fat-soluble vitamins (A, D, E, K), there is genuine risk of toxicity at very high doses. The cognitive benefit: essentially zero beyond Zone 2. The vast majority of commercial "brain supplement" or "nootropic" marketing involves taking Zone 1 evidence (deficiency correction) and misapplying it to Zone 2/3 populations (already well-nourished people).
This framework explains a persistent puzzle in the nutrition-cognition literature: why do dramatic population-level findings about iodine or iron coexist with disappointing results from omega-3 and multivitamin trials in Western populations? Because Western populations are largely in Zone 2 for these nutrients — already adequate — while the dramatic findings come from genuinely deficient populations moving from Zone 1 to Zone 2.
Dietary Patterns and Cognitive Performance
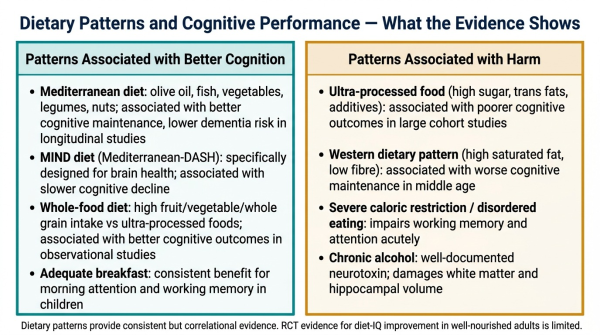
Beyond individual nutrients, overall dietary patterns are associated with cognitive outcomes, particularly in longitudinal studies measuring cognitive maintenance over years and decades:
Mediterranean diet. The Mediterranean dietary pattern — olive oil, fish, vegetables, legumes, nuts, whole grains, moderate wine — is the most extensively studied dietary pattern in the cognitive maintenance literature. Multiple large observational studies and some randomised trials associate Mediterranean diet adherence with better cognitive maintenance in older adults, lower risk of dementia, and slower cognitive decline. The mechanisms are multiple: anti-inflammatory effects, provision of key micronutrients, avoidance of ultra-processed foods.
MIND diet (Mediterranean-DASH Intervention for Neurodegenerative Delay). A dietary pattern specifically designed to target brain health, combining Mediterranean and DASH (Dietary Approaches to Stop Hypertension) principles with particular emphasis on foods with strong brain-health evidence (green leafy vegetables, berries, nuts, fish, whole grains). Observational studies associate MIND diet adherence with significantly slower cognitive decline in older adults.
Ultra-processed food consumption. Multiple large cohort studies associate high ultra-processed food consumption with poorer cognitive outcomes — including a widely cited Brazilian cohort study (ELSA-Brasil, 2022) associating ultra-processed food intake with faster cognitive decline. The mechanisms may include displacement of nutrient-dense foods, direct effects of additives, and inflammatory effects.
Breakfast consumption. The evidence for breakfast's effect on immediate cognitive performance — particularly attention and working memory in children — is consistent across multiple reviews. The effect is acute (affects the morning's performance) rather than permanently increasing IQ, and is largest in children who are nutritionally marginal or food-insecure.
What This Means in Practice
Synthesising the evidence into practical guidance:
For pregnant women and infants: adequate iodine, folate, iron, DHA, choline, zinc, and B12 during pregnancy and early childhood are genuinely important for optimal brain development. The evidence for iodine and folate is the strongest and most actionable. Prenatal vitamins and dietary attention to these nutrients during pregnancy are among the highest-value nutritional decisions in terms of child cognitive outcome. These are not supplementation-above-adequacy situations — they are prevention of deficiency during critical windows.
For children: regular breakfast, adequate iron and iodine intake, and a generally nutrient-dense diet support cognitive performance. Identifying and correcting iron deficiency anaemia specifically is well-evidenced as improving cognitive outcomes.
For already well-nourished adults: the evidence for specific supplements improving IQ or cognitive performance is weak. The primary priority is maintaining nutritional adequacy — including vitamin B12 (at risk with vegan diets), vitamin D (at risk with low sun exposure), and iron (particularly for women of reproductive age). A Mediterranean-style dietary pattern is the best-evidenced overall approach for cognitive maintenance over time. Avoiding severe caloric restriction and high chronic alcohol intake are the most cognitively protective dietary behaviours for most adults. For related context on cognitive performance, see our guide on sleep and IQ.
Nutrition has some of the largest documented effects on cognitive ability of any known factor — but almost entirely through deficiency prevention rather than enhancement above adequacy. Iodine deficiency can cost 12–13 IQ points on average in affected populations; correcting it through salt iodisation is one of the most cost-effective public health interventions in history. Iron, folate, DHA, B12, zinc, and choline all play essential roles in brain development during critical windows. For already well-nourished adults, the evidence for specific supplements improving IQ is weak — the priority is maintaining adequacy, not supplementing above it. The brain, like every other organ, needs what it needs. Beyond that point, more is not better.
For more on what affects cognitive performance, see our guide on sleep and IQ. For context on the IQ scale, see our IQ scale explained. Take our free IQ test — no registration, results in under 20 minutes.
Frequently Asked Questions
Does nutrition affect IQ?
Yes — significantly during early development, and modestly in adults. The most documented example: iodine deficiency is associated with an average 12–13 IQ point reduction in affected populations. Iron deficiency anaemia in early childhood also impairs cognitive development. In already well-nourished adults, correcting deficiencies improves performance, but supplementing above adequacy typically does not.
What nutrient has the biggest impact on IQ?
Iodine has the largest single documented nutritional impact on population IQ. It is the leading preventable cause of cognitive impairment worldwide (WHO). Severe deficiency during pregnancy is associated with 12–13 point IQ reductions in children. Salt iodisation programmes have reversed population-level IQ deficits in multiple countries.
Does eating breakfast improve IQ?
Eating breakfast improves short-term cognitive performance — particularly attention and working memory — on the morning it is eaten, especially in children. This is an acute effect, not a permanent IQ increase. The benefit is largest for children who are nutritionally marginal or food-insecure.
Does omega-3 improve IQ?
DHA (the key brain omega-3) is essential for brain development, and adequate intake during pregnancy and early childhood is associated with better neurodevelopmental outcomes. However, omega-3 supplementation in already well-nourished populations shows modest and inconsistent effects on IQ. The benefit is clearest in populations with genuine dietary inadequacy.
Can diet increase IQ in adults?
For already well-nourished adults, the evidence for diet increasing IQ above baseline is weak. The primary nutrition-cognition priority for adults is maintaining adequacy (B12, vitamin D, iron) and avoiding harmful patterns (chronic alcohol, ultra-processed food excess). A Mediterranean-style dietary pattern is best-evidenced for cognitive maintenance over time.

Comments
Share Your Thoughts